(The Lack of) Evidence on COVID-19 Suppression Measures
In lieu of randomised control trials; data is increasingly showing that lockdown policies appear to be ineffective but cause substantial unforeseen harm. Less virulent infections like flu remain in circulation despite lockdown measures and lockdown severity is correlated to increased excess deaths.

Science exists as a tool to answer questions; this not only requires a robust mechanism for assessing scientific literature, but also robust experimental design.
With COVID-19 lockdowns, decisions made on the basis of the balance of probabilities have instead been branded as "scientific" with poor communication on the potential harms and benefits. Instead of robust Randomised Control Trial evidence for public health interventions, society has been left with political discourse and distrust.
Observational data is increasingly showing that lockdown policies appear to be ineffective whilst causing substantial unforeseen harm.
This story seeks to summarise the significant lack of scientific evidence on the benefits/harms of lockdown policies (including social distancing and mask wearing).
Evidence-Based Medicine & Lockdown Policy
When commenting on scientific research, people often consider the validity in terms of adherence to the scientific method; for example, whether a paper has been peer-reviewed or is a pre-print. Fundamentally, there is another key distinction at play with Evidence Based Medicine. Systematic Reviews of Randomised Control Trial results are seen as the gold standard for experimental design, with other forms of evidence being of lower quality. On treatments during the COVID-19 pandemic, we have seen results from Randomised Control Trials which are in contrast to those seen in weaker observational studies (and some even retracted).

Dr Zoë Harcombe has noted that: "that no randomised controlled trials on spatial separation of at least one meter have ever been undertaken. None of the systematic reviews have been able to include any ’cause and effect’ studies, therefore." Zoë further notes that: "Politicians say that they are following the science. There is no science on social distancing; not as it pertains to what they are instructing us to do."
Chu et al in The Lancet also noted that there was a lack of Randomised Control Trial evidence for physical distancing, face masks and eye protection: "Robust randomised trials are needed to better inform the evidence for these interventions, but this systematic appraisal of currently best available evidence might inform interim guidance."
The Data on Lockdown Policy
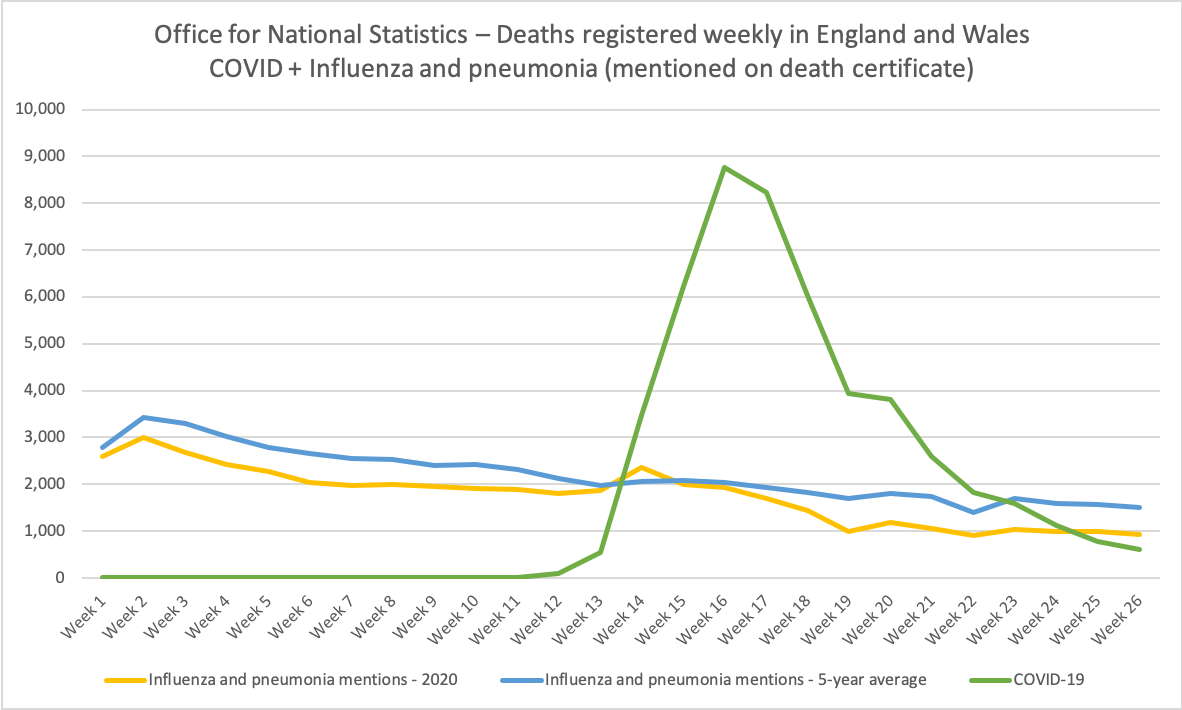
Data from the UK's Office for National Statistics indicates that there is no noticeable downturn in deaths for influenza and pneumonia on death certificates for 2020 compared to the 5 year average - and certainly none which correlates with the decrease in COVID-19 from circulation, despite flu claimed to be less virulent than COVID-19. This is even more shocking given that during the pandemic, doctors are increasingly likely to miss flu and COVID-19 co-infection and wrongly attribute other causes of death to COVID-19 (see Oxford's Centre for Evidence Based Medicine on the discrepancy between COVID-19 mentions on a death certificate versus deaths with a positive test):
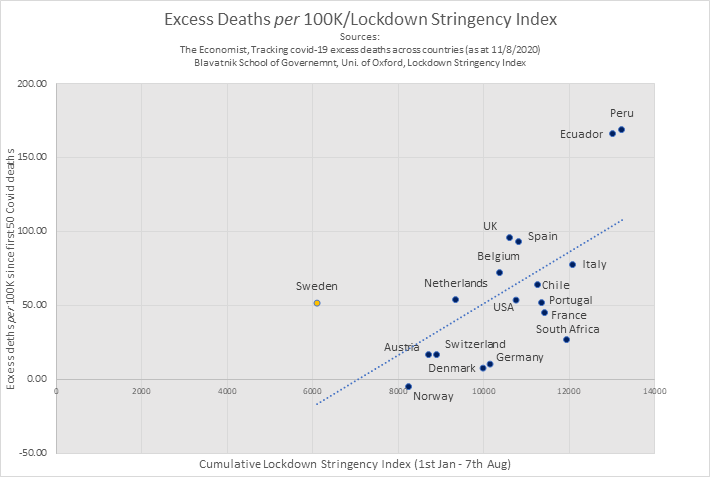
Simple observational data so far indicates that as cumulative lockdown stringency increases, so does the number of excess deaths in a country:
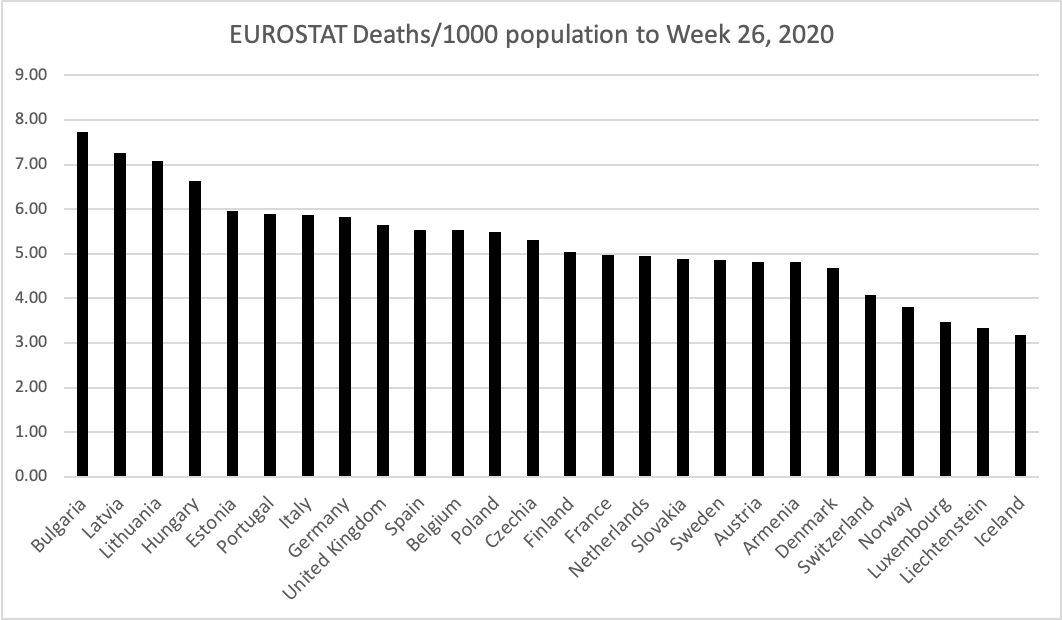
Whilst measures so far have been using flawed "COVID death" or "excess mortality" data, All-Cause Mortality shows a very different picture. EUROSTAT All-Cause Mortality data indicates that countries such as Portugal and Germany (often credited for acting quickly and decisively) have higher overall death rates than the UK or Sweden.
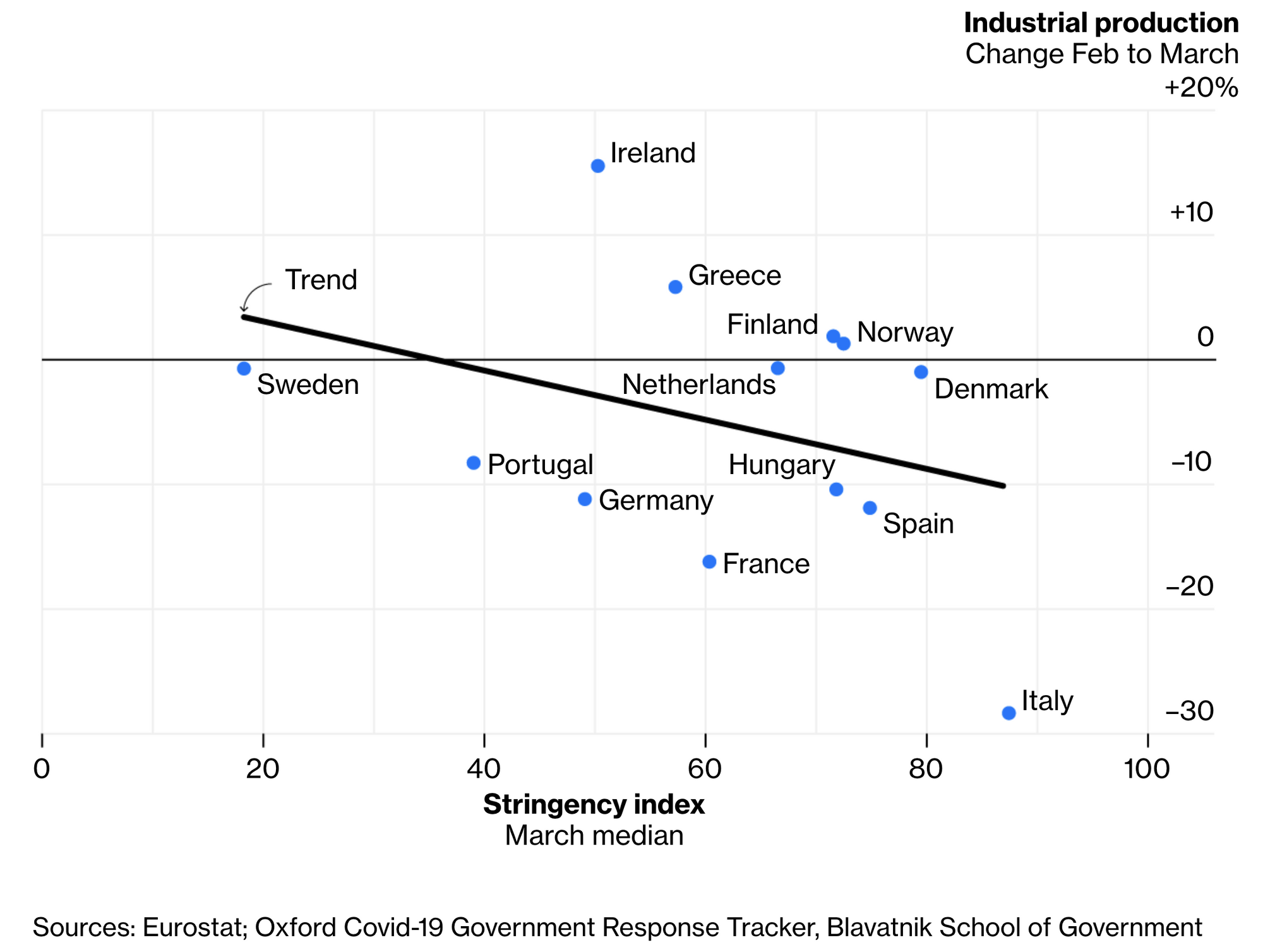
Work by the University of Oxford’s Blavatnik School of Government has found that early data indicates countries with harsher responses to Covid-19 also suffered more economically.
Negative Impacts of Lockdown Policy
There have been numerous reports indicating the significant negative effects of lockdown policy against COVID-19 deaths.
A UK government report indicates that there will be up to ~15,000 deaths from economic recession, suicide, domestic violence & accidents at home in the short-term (and up to 200,000 over the long-term in total for all reasons). In the US, one study that predicts ~75,000 deaths from drugs, alcohol and suicide.
Below are some of the other negative impacts of lockdown which have so far been recorded:
Mental Health
- Depression among UK adults has doubled during pandemic.
- Poor nutrition and less physical activity during lockdown, had a serious impact on mental health in England, according to preliminary findings from an Oxford University study.
Excess Deaths
- The British Medical Journal noted that the “Staggering number” of extra deaths in community is not explained by covid-19 with 2/3rds of excess community deaths being non-COVID.
- The British Heart Foundation noted a 50% decrease in A&E attendance for heart attacks.
- The British Medical Journal noted “striking reductions” are seen in number of people with symptoms seeking help.
- A study in the US, used data from the Denver Health Paramedic Division found that "the excess in OHCA [out-of-hospital cardiac arrests] was greater than the number of patients who died with COVID-19 diagnoses during the same time frame".
- Oxford University's Centre for Evidence Based Medicine has noted that there remains a huge excess of home deaths (even as overall death rates fall below average levels), with the vast majority of excess home deaths being unexplained by COVID.
Social Justice
- UK Chief Medical Officers state the risk to children from COVID-19 is small, whilst the risk of missing school is substantial: "This has to be set against a certainty of long-term harm to many children and young people from not attending school."
- The Deputy Chief Medical Officer for England has stated that the risk of death from flu or road accidents is higher than COVID-19 for schoolchildren.
- Kim et al in The Lancet noted that "lockdown represents a risk factor for increasing alcohol consumption in people with alcohol use disorders and relapse for those who were previously abstinent".
- A paper from the London School of Economics notes an 11% increase in calls about domestic abuse due to lockdown.
- More than two-thirds of people surveyed in 20 African countries said they would run out of food and water if they had to stay at home for 14 days.
- A report by Oxfam found that COVID-19 linked hunger could cause more deaths than the disease itself.
Impact On Research
Furthermore, the lack of cases in the UK has had a negative impact on the ability to deliver treatments for the world. If lockdown measures are successful, this could mean that they may be considered selfish for an individual country (particularly where social distancing is impossible in many countries). Researchers for the University of Oxford's vaccine for COVID-19 have noted that a fall in COVID-19 is making vaccine research harder and delaying results from efficacy trials. Furthermore, a lack of cases delays the ability of clinical trials to deliver treatments that can save a disproportionate number of lives around the world; for example, approximately 650,000 lives will be saved over the course of 6 months due to the discovery of Dexamethasone by the NHS/Oxford RECOVERY trial alone - almost 16 times the UK death toll.
Face Coverings
As countries increasingly seek to make face masks mandatory, there is a lack of Randomised Control Trial evidence as to the risks or harms of wearing face masks. This lack of evidence is noted by the University of Oxford's Centre for Evidence Based Medicine: "The increasing polarised and politicised views on whether to wear masks in public during the current COVID-19 crisis hides a bitter truth on the state of contemporary research and the value we pose on clinical evidence to guide our decisions."
Aside from the risk of infection - there is scientific evidence demonstrating that face coverings can play a role in affecting social cohesion and crime rates. One Randomised Control Trial involving children wearing Halloween masks found that face coverings can “can serve to elicit a state of deindividuation”, lower restraints and increase antisocial behaviour. Another observational study found a positive relationship between mask wearing and aggression.
Risk/Reward Benefit
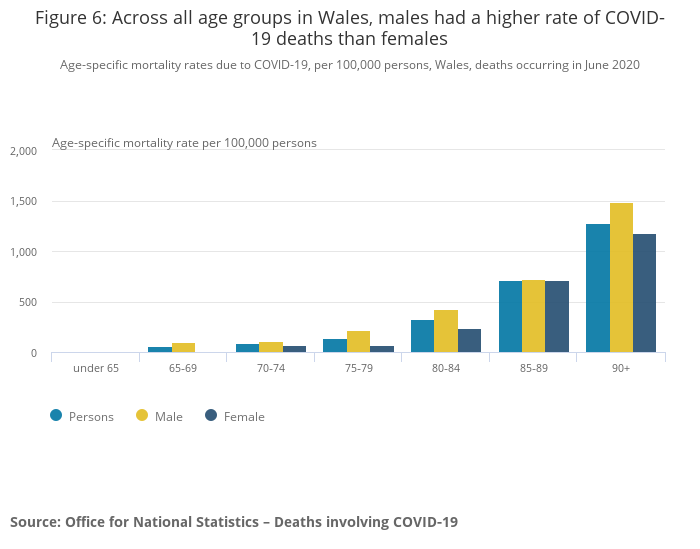
Whilst COVID-19 has a disproportionate affect on the elderly (note in the chart below deaths are negligible in the under 65 group), it is not understood how lockdown policy measures affect mortality across different age groups or the number of life years lost overall. In effect, greater harm could be done to those with a many life years left at the expense of those with very little life years lost:
Without Randomised Control Trials to answer questions on the benefits and harms of lockdown policy, policy makers must make policy on the basis on the balance of risk and reward.
Whilst scientists exist to formulate experiments to answer questions and doctors exist to treat patients, engineers (including those in areas involving infection control) exist to build complex systems. Engineering Council UK, the regulatory body of engineers within the UK, provides in its guidance on risk management that it is essential to "assess the balance of risk and reward" alongside effective communication: "Society’s perception of risk may differ from the engineer’s, and therefore engineers should strive for clarity when communicating about risk, and communicate in terms understandable by non-specialists."
Modelling work on the COVID-19 pandemic was not validated on experimental data or subject to peer-review and therefore not scientific, but also not subject to appropriate engineering oversight. Risk management not only failed in the software engineering of such models, but also critically did not account for the harm caused by the interventions proposed within them.
Conclusion
When valid scientific questions have been asked on treatment or vaccine candidates, science does what it is there to do - answer questions. Where there is substantial scientific uncertainty (on lockdown measures or face masks), instead of forming scientific evidence to answer such questions, we have been left with political dogma. It therefore seems that scientists are exceeding their area of competence in designing interventions where huge amounts of uncertainty exist. This combined with ineffective communication and fear-mongering has harmed the effectiveness that any such interventions may have.